
{kind=link}
The framing effect
How we perceive numbers depends on how they are framed. We view a treatment that has an 20% chance of failure less favorably than one that has an 80% chance of success. Of course, there’s no difference between these treatments.
Quote 1
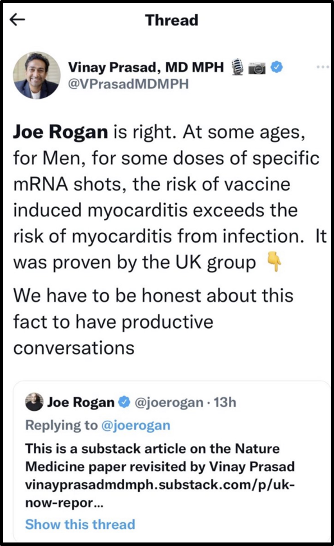
With this in mind, let’s examine two quotes by Dr. Vinay Prasad. The first of these was a tweet where he commented on vaccine-myocarditis. He said:
No one says “vaccine induced myocarditis is mostly mild” like someone who just saw a graph that 20% of people 37 weeks later have not fully recovered. We are talking healthy boys who are mostly getting a 2nd or 3rd dose here. Truly unacceptable.
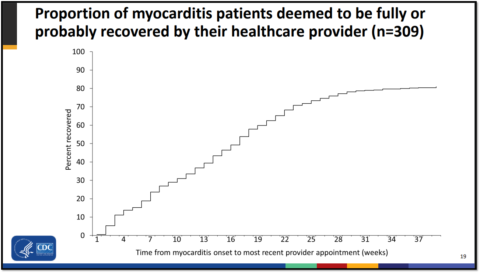
While Dr. Prasad was correct that vaccine myocarditis usually occurs in teenage boys after their second-vaccine dose, he was wrong to say all affected boys were all healthy. Given the high obesity rates in the US, tens of millions of children have a risk factor for severe COVID. He was also wrong about the risk of the third shot, which is about 1 in 100,000. However, his “20% of people 37 weeks later”, taken from the graph below, was right.
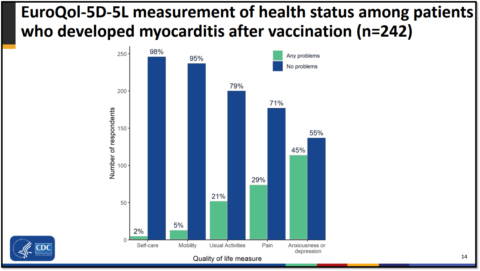
According to the CDC, 80% of children who develop vaccine myocarditis fully-recover, while 20% of have persistent symptoms, most commonly anxiety/depression. Other symptoms include pain, fatigue, shortness of breath, and palpitations (slide 13). A very small number of children are more impaired. Hopefully they will recover fully over time, but it’s possible some may not. Additionally, affected children will have to be monitored over the long-term to evaluate for cardiac scarring. The CDC (slide 30) stated that ‘To our knowledge, there were no vaccine-associated myocarditis deaths in this group”, and Dr. Frank Han previously explained why such claims need to be carefully evaluated.
Let’s dive into these numbers a bit further with some back-of-the-envelope calculations. The incidence of vaccine-myocarditis, which I summarized here, is hard to pin down, as different studies from around the world have given different results. One preprint found a rate of 1 in 2,650 for adolescent boys, while another study found the rate was 1 in 52,300. One study from Denmark found no increased risk for males at all, while a meta-analysis pinned the rate at 1 in 7,000-20,000 with “low certainty”. Though the exact rate is not known, a reasonable estimate is that it occurs in 1 in 10,000 adolescent boys after their second Pfizer dose. Since 80% of children recover, the rate of an adolescent boy getting and not fully recovering from vaccine-myocarditis after 37 weeks is about 1 in 50,000.
According to the American Academy of Pediatrics, about 7.2 millions boys ages 12-17 have received two vaccine doses (slide 4). This translates to 720 cases of vaccine-myocarditis in boys this age in the US. 576 of them have “fully or probably recovered,” while 144 have “improved, but not fully recovered”. As perhaps 30,000 teenagers are getting their second shot on a weekly basis, this means there are 1-2 new cases of vaccine-myocarditis every week, though this number is plausibly zero if pediatricians are spacing out the two doses. As such, I am confident the number of times many doctors, including myself, have discussed this side effect greatly exceeds the number of children who are currently hospitalized with it.
Nonetheless, I’m on record as saying:
It’s serious anytime a young person gets admitted to the hospital, even if they leave after a few days feeling well, as most seem to do.
I stand by this, and I’ve always maintained that vaccine-myocarditis should not be trivialized.
Quote 2
Dr. Prasad’s second quote came from a podcast from 2/4/2021 where he argued against the Emergency Use Authorization for pediatric vaccines. He said:
So of all the people who’ve been infected the probability one would die, when we’re talking about ten-year-olds the estimates that are in this paper is something like 2 in 100,000. So that’s of 100,000 kids infected maybe 2 would pass away. And to put that in perspective, when you talk about people who are 80, it’s 7,500 times as much.
When Dr. Prasad made that statement, 227 children had died of COVID, according to the American Academy of Pediatrics, which collected data from 43 states and NYC. That grim death tally now stands at 1,700 children, per the CDC. This means that 1 in 44,000 children have already died of COVID in the US. Considering that most but not all children have had COVID, or many had it after having been vaccinated, the true death rate for unvaccinated children is slightly higher than this. However, the risk is not the same for all children. Babies have the highest death risk by far. As such, Dr. Prasad’s estimate that 1 in 50,000 10-year-olds who get COVID will die of it sounds accurate to me. All children have an extremely low risk of dying thankfully. Of course, he’s also right that 80-year-olds have a much higher risk of dying.
So by my rough but reasonable estimates, the number of children killed by COVID (1,700) is 12 times larger than the number of children with persistent symptoms after vaccine-myocarditis (144). The number of adolescent boys killed by COVID (380) is 2.5 times larger than this. Of course death is not the only negative consequence of COVID. Beyond many millions of children feeling sick to varying degrees, the number of children hospitalized by the virus is about 200 times greater than the number hospitalized by vaccine-myocarditis. Some of these children are very sick, needing mechanical ventilation in the ICU. Given that the vaccine has been shown to limit these rare but severe outcomes in multiple studies, I have no doubt the vaccine has prevented much more suffering than it has caused.
That’s all that really matters and yet, it’s controversial.
Two interesting things and some advice
I now want to point out two interesting things. First, the risk of a child dying from COVID is basically the same as an adolescent boy getting and not fully recovering from vaccine-myocarditis. Second, Dr. Prasad, framed these two adverse outcomes very differently, and he’s done this the entire pandemic.
He mocked the idea that “vaccine induced myocarditis is mostly mild”, even though 80% of children recover. He said the 20% risk of persistent symptoms was “truly unacceptable”, even though this translates to about 1 in 50,000 adolescent boys. This rate of persistent side effects really bothered him. Me too. It’s terrible that some children might have been better off had they not been vaccinated. Even though the risk is super low, these children matter.
However, Dr. Prasad’s framing of pediatric fatalities was quite different. Did he deem 1 in 50,000 children dying of COVID as “truly unacceptable”? No, he did not. In fact, he felt this death rate needed “perspective”. He could have pointed out that in the pandemic’s first year, a single child died of the flu, while COVID killed over 200 children. However, this “perspective” would have made the pediatric death toll seem high, and Dr. Prasad doesn’t want to do that. This is why he’s literally devoted a dozen podcasts to vaccine side-effects, but none to children lost to COVID or the many studies showing the vaccine can benefit them.
When dealing with pediatric deaths, Dr. Prasad instead chose to minimize this risk by stressing that elderly people have it worse. He used the salesman’s trick I discussed previously, where a large, irrelevant number – in this case that elderly people have 7,500 times the risk – is juxtaposed against a child’s risk, to minimize the virus’s impact. The goal is to convince people it’s OK if a relatively small number of unvaccinated children suffer or die from COVID so long as grandma suffers more. This makes no sense, and is formally known as the fallacy of relative privation (discussed here and here).
While it’s true that elderly people have a much higher risk than children, reasonable people understand that a child’s risk is independent of how it affects older people. COVID wouldn’t suddenly be worse for children adults were spared. 1,700 children have died no matter what the virus did to grandma, and too many of them perished after the vaccine was available to them. Normal people think that’s sad and want zero children to suffer or die for lack of a vaccine.
Dr. Prasad seems to imagine zero children have suffered or died for lack of a vaccine, though of course some have. At times, he doesn’t even acknowledge children can die at all. I guess bringing up that COVID can do much more than cause myocarditis precludes honest and productive conversation? (Rogan was wrong.)
“Any strong advocate for kid covid vaccination is off their rocker. It really doesn’t matter. The risks are super low.”
To his credit, I suppose, Dr. Prasad dropped all the pretenses, and is no longer arguing that children don’t need the vaccine because COVID is going away, because the vaccine causes fevers, because grandma is at more risk, or any of the other spurious reasons he’s given in the past. Now he is now very open that children gravely affected by COVID really don’t matter. He recently said pediatric vaccine-advocates were psychotic, tweeting that,
Any strong advocate for kid covid vaccination is off their rocker. It really doesn’t matter. The risks are super low.
I had to check to make sure he really said that. The argument seems to be, “Kids don’t need the vaccine, just because“.
Everyone agrees with Dr. Prasad that the risks are super low. This is not a deep insight. But a super low event multiplied by many millions of infections adds up. This seems like a very simple concept to me, and I don’t think over 1,500 dead children in two years is nothing.
Do you?
The risk of a child getting shot is super low, but guns are the number one cause of death in children. Because the risk to any individual child is low, does this imply a child killed by a bullet “really doesn’t matter”? Does it mean that any “strong advocate” to reduce gun deaths in children is “off their rocker”? Should we have fences around pools and airbags in cars? Should anyone bother trying to save any child from anything? After all, the risk of that particular thing is probably super low.
Around 20,000 children die each year in the US. These are the real questions then:
- Should we bother trying to stop 5% of the deaths?
- If not, what is the magic number of dead children where we should suddenly start to care and say, “Hey, maybe we should try to stop this“?
I don’t know the answers, but 5% seems a big enough number to me, even though, yes, 95% of pediatric deaths are from some other cause.
Sadly, there is no vaccine for bullets, accidents, and suicides. I wish there were, though assuredly some doctors would oppose these imaginary vaccines because the risks they defend against are “super low”. However, of the leading causes of death in children, only COVID can have its already low risk lowered with 3 simple shots.
Why not use them? Why not help some children, even if that number isn’t that large? The vaccine reduces pediatric hospitalizations, though not perfectly. Arguing against the vaccine for this reason is the Nirvana fallacy, which is a standard anti-vaccine talking point.
We all get that only a few kids will really benefit from the vaccine. Again, this is not a deep insight. It astounds me that people think is a valid reason not to use the vaccine, yet, I hear it all the time.
“Wow, this quack is the head of an institute of an actual medical center?”
Prior to the pandemic, Dr. Prasad called a doctor a quack because he fear mongered about the flu vaccine. What exactly did that doctor say, I wonder, to make Dr. Prasad earn such a stern condemnation? Why has Dr. Prasad’s attitude shifted, even though COVID has killed more children this year than every vaccine-preventable disease combined.
If you’re against the COVID vaccine, then how would you argue with an anti-vaxxer who opposed the MMR, polio, and diphtheria vaccines? After all, the risk of those diseases for any individual child in American is super-duper low. “It really doesn’t matter“, the anti-vaxxer would say. And while these diseases are currently held at bay only by vaccines, the anti-vaxxer would be more right than someone who said COVID doesn’t really matter. COVID is the virus that is threatening American children right now. If a parent were only willing to give their baby just 1 vaccine this year, I’d suggest the COVID vaccine in a heartbeat.
What other reasonable choice is there?
“The US should suspend all vaccination in children under 18”
Additionally, I’d call Dr. Prasad a strong advocate of speaking out about vaccine-myocarditis. He opposed the initial authorization of the pediatric vaccine. Later, Dr. Prasad was so concerned about vaccinated-related myocarditis he thought last year “that the US should suspend all vaccination in children under 18 and give only one dose of vaccine to men under 25”. Imagine how much suffering was prevented because regulators with skin in the game paid this no heed. As stated above, Dr. Prasad has over dozen YouTube videos on the subject and he’s Tweeted about it constantly. He’s said things such as, “I don’t think people realize the damage continuing to push two doses in young men will do”. His name is associated with vaccine-myocarditis the way Michael Jordan is with basketball.
So why has he chosen to be such a strong advocate for something with a “super low” risk? If those advocating to keep children safe from COVID are “off their rocker”, what should be said about those who work to keep them safe from the vaccine? Does he think vaccine myocarditis is worse that death?
Dr. Prasad’s “really doesn’t matter” attitude contrasts very sharply with doctors who have real-world responsibility for sick children. Pediatricians have seen what the virus can do and they are alarmed at low vaccination rates. To pick one example amongst many, Dr. Mobeen Rathore, a Florida pediatrician said during that state’s Delta wave,
Kids do get sick. Kids do get hospitalized. Kids do get sick and go to the ICU get intubated, be on a ventilator and even be on ECMO which is a heart lung machine, sort of a last ditch effort to support these children. Unfortunately children do die. In fact many of you probably heard the news, there’s a 17-year-old who died in St. Johns County just in the last few days so I think we have to be very sure and understand that kids can get serious illness. And I can tell you that in the almost 18 months ending in June we had three deaths in our area in children. That’s one death every six months. And just in July and August we had four deaths in children so that’s two deaths a month.
I’d be surprised if there was a single pediatric ICU doctor in the US who shares Dr. Prasad’s nonchalance on this subject. Dr. Rathore, a pediatrician in an anti-vaccine state, Florida, recognizes:
This could result in some children dying.
“All children should be vaccinated,” he says. “This is the only way we’re going to get out of this morass of the pandemic”.
The advice
Now for the advice. Pay attention and read critically. Misleading framing is everywhere. When reading about COVID and children, try to be aware of how the author is framing the information they are sharing. This includes me, and I’ve worked carefully on framing in this article. Are you given raw numbers so you can form your own opinion about whether a harm is “rare”, “frequent”, “mild”, or “severe”? Or is the author trying to lead you in one direction with strategic omissions rhetorical sleight of hand? Are you being presented with an informative and nuanced perspective? Or are you instead reading the work of a sheltered contrarian doctor – and there are many – who frames data in an attempt to trick you into thinking vaccine side-effects are worse than death?